| | | | | | | | | | | | | | | | On behalf of my colleagues at MROCC it is my pleasure to welcome you to the inaugural edition of the MROCC MRO Quarterly Newsletter. At the outset I would like to join Dr. Doug Martin in honoring Dr. Robert Swotinsky for his almost 3 decades of leadership as editor of the ACOEM MRO Update. Equaling the excellence of his journal is a high bar that we will strive to maintain. I would also like to thank Dr. Martin for his willingness to allow MROCC to assume the responsibility of this newsletter publication and because of his awareness of the need to keep MROs up to date and informed, his agreement to join our list of contributors. Contributors to our inaugural issue are some of the most well known and experienced experts in the field of drug testing. I want to thank them all for their efforts, and to invite submissions from our readership of thoughts, questions, papers and comments that would be of general interest to MROs in all aspects of MRO responsibility and the review of laboratory results. We want this journal to be yours as well as ours and we look forward to ongoing fertile exchanges of ideas. Finally I’m happy to let everyone know that we have expanded our Board of Directors at MROCC and I would like to welcome 3 new members: Dr. Douglas Martin Dr. Gina Pervall Dr. Neha Badheka They will be joining Dr. Kent Peterson, Dr. Ben Gerson, Dr. Chuck Prezzia, Dr. Steve Taylor, Dr. Ken Lankin and myself on our Board. MROCC has always been an organization of physicians for physicians. Please feel free to reach out to the MROCC office (
mrocc@mrocc.org) with questions or comments. |
|
|
|
|---|
| |
| | | | | | | | | | | | | | | I am pleased to be a part of the inaugural edition of the MROCC MRO Quarterly Newsletter. As many of you know, for more than two decades, the American College of Occupational & Environmental Medicine (ACOEM) published the MRO Update Newsletter. MRO Update’s focus initially was to educate MROs on their role, especially since the function and position was only created in the late 1980s by federal statute. Over the years, the MRO Update instructed and kept us informed regarding changes to the federal drug testing statutes, made us aware of state non-federal drug testing trends, and provided us with reports on legal case outcomes that were relevant to MROs and their practices. However, as the MRO field matured, interest in the newsletter and its subscriptions began to decline. It was also clear that not all certified MROs necessarily turned toward an ACOEM publication for updates to the field, as not all MROs are occupational physicians. ACOEM faced a dilemma as to whether to continue to sponsor a newsletter that had fewer subscriptions but continued to be costly to create and distribute. This did not mean that ACOEM had any less interest in MROs or the field of drug testing. The MRO Section, which has typically been the Section within the College that had the largest membership, and for which I was honored to lead as Chair for 20 years, continued to be active and continues to be a valuable resource. To address the decline in subscriptions, many different options were explored. After weighing these options, it was determined that our strategic partner at MROCC would be the natural and appropriate group to take over such a newsletter. As we are at the forefront of welcoming oral fluid testing into the federal drug testing process, it is time again to ramp up education and communication to certified MROs so that they have the tools necessary to perform their tasks in the most efficient and accurate manner. It is our hope that the MROCC Newsletter will continue the good guidance and timely communication about areas that MROs must keep current with. ACOEM is particularly pleased that MROCC has taken on this task and will support their efforts going forward and we are excited about the future of our collaboration. ACOEM continues to be focused on its MRO members and will continue to offer a collegial atmosphere, sounding board, and peer group access point for MRO questions and concerns. Both personally and on behalf of ACOEM, we would like to thank Dr. Robert Swotinsky, who served as editor of the MRO Update newsletter from its inception. Dr. Swotinksy has provided an enduring service to MROs over the years, and it is not possible to place a value on what he has brought to the field because of his tutelage and guidance. |
|
|
|
|---|
| |
| | | | | | | | | | | | | | | | | QUESTION: For purposes of verifying a drug test, how old can a prescription be and still be valid? ANSWER: This question of “what is a valid medical explanation” is commonly raised by MROs. The answer requires a bit of explanation. WHAT IS A VALID PRESCRIPTION? Among dozens of definitions that I found, only one specified any time limits.(1) “Valid prescription means a prescription written by a licensed health care practitioner who is authorized by law to prescribe medicine and is presented within 12 months of the date the prescription was written, except for controlled substances which must be presented within six months of the date written.” However, the answer depends on whether the drug is a controlled substance, and upon state laws. Under federal law, there is no time limit on filling schedule II drugs, such as methylphenidate (Ritalin®). However, many states have laws that limit the time, along with limiting the amount of drug a pharmacist can dispense. A prescription for a drug in schedules III or IV is valid for six months after being written. HOW LONG CAN A PRESCRIPTION BE REFILLLED BEFORE IT EXPIRES? Note that these definitions do not include a time limit for how long the drug may be taken. However, some guidance may come from how long a patient has to refill a prescription. Once a prescription for a non-controlled drug is filled, it is valid for a year after the filling date in most states. Some states have extended this period up to 24 months. If your doctor includes refills on your prescription, you have one year to use them. Prescriptions for schedule II drugs aren’t refillable. Schedule III and IV prescriptions are valid for six months after you fill them. If your doctor provides refills, you have six months to use them. Federal law limits the number of refills in that timeframe to five. HOW LONG DOES A PRESCRIBED MEDICATION REMAIN LEGALLY VALID? Various possible sources of information may provide guidance that might be useful to an MRO in determining how OLD a prescription can be and still represent a legitimate medical explanation. - Prescription bottle: Most prescriptions have an expiration date on the bottle typed by the pharmacy. These dates usually run from 6 to 12 months from the time of issuance. This partly reflects standard pharmacy practices, the estimated average active shelf life for a medication, as well as encouragement for the individual not to use the medicine long after it was prescribed. In fact, some medications have a short life, e.g., epinephrine, nitroglycerine, or some antibiotics; others such as opiates remain pharmacologically active for many years. For example, a military study of stockpiled medications showed that 90% of more than 100 drugs, including prescription and over the counter, actually performed perfectly well even 15 years after the expiration date! So the prescription bottle is essential to verify that a prescription was issued, but not helpful to the MRO in determining how long a prescription may be taken.
- Prescribing health professionals. PLHCPs rarely specify an expiration date in their medical records, either on prescriptions or how long the drug can be used. However, an MRO may want to request copies of pertinent sections of a written medical record from the prescribing healthcare professional. In my experience these have seldom been helpful to the MRO with regard to duration of medication use.
- U.S. Drug Enforcement Administration (DEA), Department of Justice: The DEA has declined to set a duration at which the use of one’s own prescription constitutes illegal use. The DEA defines a valid prescription under the Controlled Substances Act (CSA) of 1970. A Q&A states: “In order for a prescription for a controlled substance to be considered valid, it must be ‘issued for a legitimate medical purpose by a registered practitioner acting in the usual course of sound professional practice.’ ” The specified information that must appear on a valid prescription includes “directions for use” but does not include the duration for which the medication can be used.
- Substance Abuse and Mental Health Services Administration (SAMHSA): SAMHSA’s 2018 update of their Medical Review Officer Guidance Manual for Federal Workplace Drug Testing Programs addresses MRO review of drug test results for federal employees. Section 4.5.3 states: “when determining whether a legitimate medical explanation exists for a positive test, the MRO should consider whether a medication was used during the time period for which it was legitimately prescribed, if such a time period is specified. If a donor possesses a valid prescription with no time limitations on the drug’s use (even if the dispensed prescription is past its expiration date), the donor’s specimen should be reported as negative.” So if an MRO believes the donor is taking medication beyond the time period for which it was prescribed, they should report a negative drug test, but add a safety concern in their communication to the donor’s federal agency.
- U.S Department of Transportation (DOT): At one time, the Federal Motor Carrier Safety Administration (FMCSA) website did state in a Q&A that a prescription should be no more than a year old. However, this was never DOT policy and that Q&A was removed years ago.
DOT’s written response in 2017 to comments received about the proposed addition of semi-synthetic opioids clarifies the DOT’s position.(2) “The DEA has not set a maximum duration for the length of time a prescription can be considered to be legally used by the person to whom it was prescribed. Consequently, it would not be appropriate for the Department to substitute its judgment for that of the DEA, which is the Federal agency with the authority for determining what constitutes a valid prescription under the CSA.” “The MROs are highly qualified individuals who Part 40 requires to make judgment calls. MROs must take into account differences in medications, and other case-specific factors. While some commenters characterize this as ‘‘inconsistent’’ across the breadth of a national program, it carries out the intention that MROs will make individualized determinations for each donor. Although it might be less work and superficially ‘‘consistent’’ for MROs to make decisions on the basis of a ‘‘bright line’’ standard, doing so would not advance the objectives of the program. Consequently, the Department will not create a time limit on the use of a legally valid prescription.” “Some commenters also suggested that the final rule prohibits an MRO from questioning whether the prescribing physician should have prescribed the substance. That is, the MRO should not be allowed to say, in effect, ‘‘yes, the employee has a legally valid prescription issued by his or her physician, but I think that the physician should not have issued that prescription in the first place, or the prescription was for too high a dosage of a drug, so I won’t treat the prescription as a legitimate medical explanation for a laboratory positive.’’ This situation could arise, for example, with respect to prescriptions for the opioids added to the DOT panel by this rule (or for any other legally prescribed drug identified in our drug panel), if an MRO thought an employee’s doctor had been too liberal in prescribing pain medications.“ “We agree that it is inappropriate for an MRO to question an employee’s legally valid prescription in this way. Even if the employee’s physician’s prescription practices are inconsistent with an MRO’s understanding of good standards of medical practice, employees are entitled to rely on their physicians’ prescriptions as authorization to use the legally prescribed substance as a legitimate medical explanation.” Conclusion: Based on the above information, especially guidance from the DEA, HHS, and DOT, I recommend that MROs accept a valid prescription for medication issued in a person’s name, even if it appears outdated and perhaps prescribed or used inappropriately. If an MRO verifies a drug test as “negative,” they still have the opportunity to raise safety concerns, which should lead to the donor having a clinical evaluation of fitness for duty. REFERENCES: 1. Drug Enforcement Administration:
https://www.lawinsider.com/dictionary/
2. Department of Transportation:
Federal Register Notice for the November 13, 2017 final rule adding the semisynthetic opioids to 49 CFR Part 40 |
| | |
| |
|
|---|
| |
| | | | | | | | | | | | | | | | | | | | | | | | |
|
| |
|
|---|
| | |
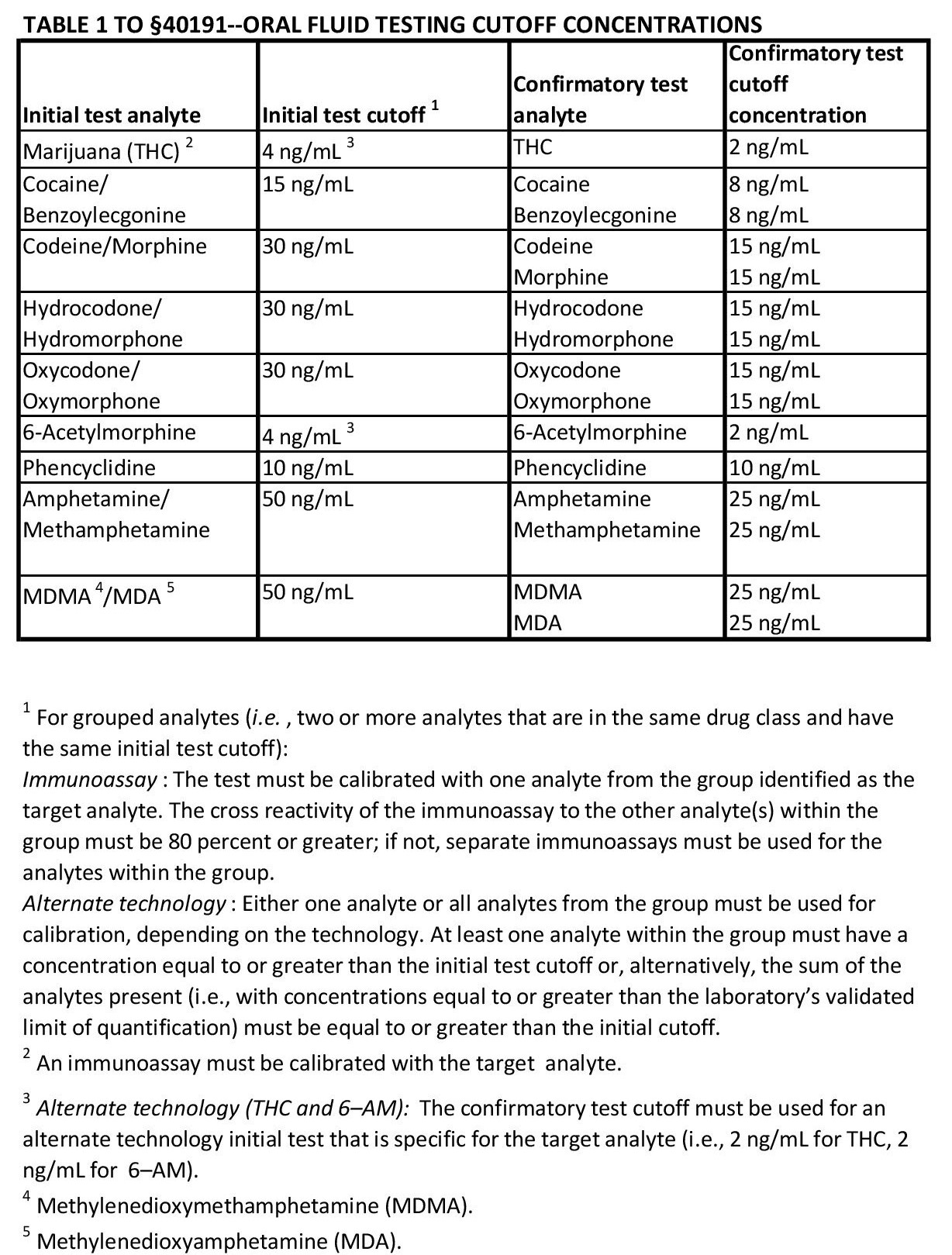
| | | | | | | | | | | The Department of Transportation (DOT) issued a Notice of Proposed Rulemaking (NPRM) on February 28, 2022 to revise 49 CFR Part 40 to include oral fluid drug testing as an option for transportation employers in fulfilling their drug testing obligations under DOT agency regulations. There was a 60-day public comment period, during which interested parties were encouraged to submit comments in response to DOT proposed changes to Part 40. A final rule is not expected until the end of 2022. Since its inception in 1990, the DOT-mandated drug testing of safety-sensitive transportation employees has been a urine drug testing program. This is the first time that employers would be able to use oral fluid specimens to deter and detect prohibited drug use under the federal rules. The DOT has stated that the primary factors impacting their decision to allow oral fluid drug testing are: 1) to combat cheating (specimen adulteration, substitution, and dilution) in urine drug testing; and 2) to facilitate testing that may be more economical and less invasive than urine drug testing. The NPRM does not end urine drug testing, but rather gives employers the option to use oral fluid drug testing in their programs—for all their testing or in certain circumstances or for specific testing events (e.g. pre-employment, post-accident, etc.). The employer’s policy would determine if, when, and where oral fluid testing would be used for its DOT-mandated testing program. The DOT-proposed procedures for using oral fluid drug testing are based on the technical, scientific, and forensic principles included in the Department of Health and Human Services (HHS) Mandatory Guidelines for Federal Workplace Drug Testing Programs using Oral Fluid (OFMG) which became effective Jan 1, 2020 for testing federal employees. DOT-mandated drug testing is tied to the HHS Mandatory Guidelines by the Omnibus Transportation Employee Testing Act (OTETA, 1991), requiring DOT-mandated testing to use procedures, technology and methodology contained in the HHS Mandatory Guidelines. The proposed revisions to Part 40 include oral fluid specimen collection, laboratory analysis, and medical review officer (MRO) procedures—all based on the HHS OFMG. Here are the highlights: ORAL FLUID (OF) SPECIMEN COLLECTION: OF collection procedures are similar to urine specimen collection. The OF collection is documented using the 2020 version of the Federal Drug Testing Custody and Control Form (CCF) which can be used for either urine or oral fluid specimens. All OF specimen collections are observed/witnessed by the collector. In the presence of the collector, the donor puts the collection device swab into his/her own mouth and then when the OF is collected, places the swab/pad into the tube/vial. OF collectors would have to complete training similar to what is required of urine specimen collectors. The OF specimen collection devices, consisting of a felt pad on a stick and a vial/tube containing a buffer/preservative solution, must be FDA approved and meet the specification outlined in the rule. The DOT additionally requires that OF specimens be collected as split specimens and is insisting that the OF collection device be configured so that the OF is subdivided into two vials/tubes using one OF collection device. There are currently no such FDA-approved OF collection devices capable of that. There is a 10-minute observed “wait period” prior to conducting the OF collection, and there are pre-collection procedures for deterring attempts to cheat on the test. The OF collection devices are tied to the screening assays and reagents used for OF testing at the laboratories, so they are somewhat “lab specific” in where the OF specimen collected can be sent for analysis. The OF collection devices cost $3-6 and have a 12-18 month expiration date – a significant difference to urine collection kits which are generally supplied by the laboratory at no additional cost and do not have any expiration date or need for inventory controls. ORAL FLUID (OF) LABORATORY PROCEDURES: The OF laboratory procedures DOT will use are the same as those in the OFMG; the same drug testing panel and cut-off levels; the same requirement for quality control and documentation (see Table I below). The cut-off levels for drug analytes in OF are much lower than those used for urine testing because there is less deposition of drugs in OF than in urine. OF testing window of detection for drug use is generally shorter than in urine (e.g. THC in OF up to 24 hrs.; in urine 3-30 days). There is no specimen validity testing required at the laboratory for OF. The laboratories must be certified/approved by the National Laboratory Certification Program (NLCP) to conduct OF drug testing for federal programs, including DOT-regulated testing. Several laboratories are in the process for NLCP approval, however, to date there are no laboratories certified for OF testing. |
| | | | | MRO PROCEDURES: The DOT proposed procedures for MRO review, interpretation and reporting of laboratory OF test results, are essentially the same as they are for urine drug testing. The results are reported by the laboratory to the MRO, using the same nomenclature as for urine testing. For codeine/morphine positive results there is a similar “secondary cut-off” value used to consider the impact of poppy seeds (e.g., an OF specimen reported positive at or above the 15 ng cut-off, but less than 150 ng/mL is attributed to poppy seed ingestion unless the donor admits to illicit, or unauthorized morphine/codeine use). The DOT proposed Part 40 revisions also include several items that would apply to both urine and OF tests: 1) permitting MRO staff members to contact pharmacies to validate prescription medications dispensed; 2) procedures allowing the MRO to “un-cancel” a DOT test when additional information is made available that would enable the MRO to report a negative, positive, or refusal to test result. And 3) additional restrictions on how the MRO reports “medication safety concerns” to employers and other authorized third parties. Two of the most significant potential impacts of DOT employers using OF testing concern the problems associated with urine drug testing “shy bladder” events and requirements for “directly observed” or witnessed urine specimen collections. The proposal suggests that employers would authorize the use of an OF specimen when a donor is unable to provide an adequate urine specimen. This could potentially eliminate the lengthy, complex and costly “shy bladder” process, including the physical examination of the donor by a referral physician and the MRO’s subsequent final test determination based on the referral physician’s findings. Another possible impact of an employer authorizing OF specimens is when a direct observation urine collection is required – either at the collection site when the donor has presented a “suspect” (e.g., temperature out of range) urine specimen and an immediate second specimen collection that is directly observed is needed; or when a previous invalid urine drug test has been cancelled by the MRO and a re-collection under direct observation is ordered; or when the test is a DOT return to duty or follow-up test which requires a direct observation specimen collection. To ease the difficulty in finding a qualified observer for witnessed urine specimen collections, the DOT is also proposing to allow exceptions to the “same gender” observer requirement in the case where the observer is a licensed/certified medical professional. The extent to which DOT-regulated employers will embrace OF drug testing is not known. Will it, by and large, replace urine drug testing? Will urine testing remain the “specimen of choice” with OF testing being an alternative in specific circumstances? Will employers be inclined to train their own personnel to serve as OF specimen collectors, possibly saving time and expense of third-party specimen collection services? Time and regulatory guidance will probably tell! ____________________________________________ Public comments on proposed changes can be reviewed at
https://www.regulations.gov/document/DOT-OST-2021-0093-0001 | | |
| | |
|
|
|---|
| |
| | | | | | | | | Barry Sample, PhD - Barry Sample Consulting, LLC and
Faye Caldwell, Esq, Managing Partner – Caldwell Everson PLLC ____________________________________________ |
| | | Changes in analytical techniques used by laboratories for the testing of amphetamines as well as increasing utilization of alternative specimen types (i.e., oral fluid and hair) warrants a fresh look at the Medical Review Officer (MRO) review of positive methamphetamine results. BACKGROUND Methamphetamine (Desoxyn®, Methedrine®) is a sympathomimetic amine, closely related to amphetamine (N-methyl derivative) and ephedrine (desoxy derivative). While amphetamine was first synthesized in 1887, it was not until 1919 that methamphetamine was first synthesized. Methamphetamine is a stimulant and has been used clinically for the treatment of obesity, narcolepsy, and (less frequently) attention deficit hyperactivity disorder since 1930. The amphetamines were purportedly used by both sides to increase the efficiency of military personnel during World War II, and as recently as the Gulf War by the US armed forces. Methamphetamine undergoes de-methylation to amphetamine and hydroxylation to p-hydroxy-methamphetamine. While the urinary excretion of methamphetamine and its metabolites are greatly influenced by urinary pH, the majority of a dose is eliminated as the parent compound – under acidic conditions, approximately 7% of a dose is eliminated as amphetamine and under alkaline conditions, as little as 2%. Both methamphetamine and amphetamine are detected in urine, oral fluid and hair after the use of methamphetamine. Consequently, the detection of amphetamine is commonly used – and required for Federally-mandated urine tests – for the laboratory reporting of a positive methamphetamine result in order to demonstrate that the positive is due to use or ingestion. This ‘amphetamine rule’ also precludes a specimen from being reported as positive due to either an artifact from ephedrine during confirmatory testing or external contamination (hair). The amphetamines have chiral centers and exist as enantiomers – meaning they are mirror images, but are not superimposable – and are classified as either d(extro)- or l(evo)-isomers based on the direction they rotate a plane of polarized light. A way to envision this phenomenon is to think of one’s right and left hand which are mirror images but not superimposable. Additionally, there is no in-vitro metabolic pathway for the interconversion of d‑ and l‑isomers. Generally, the d‑isomers have greater central (nervous system) activity while the l‑isomers have greater peripheral activity. Consequently, the d-isomers have a higher abuse potential. When first scheduled in 1970, the amphetamines were listed as Schedule III substances. Owing to their growing abuse potential, the DEA quickly moved the amphetamines to Schedule II in 1971. l-Methamphetamine (50 mg, levmetamfetamine, l‑desoxyephedrine) may be legally marketed in over the counter (OTC) decongestant nasal inhalers. LABORATORY ANALYSIS Until October 2017 with the publication (82 FR 7920) of the revised Mandatory Guidelines for Federal Workplace Drug Testing Programs, all federally-mandated initial testing for drugs was required to be performed using immunoassay. Since then, initial testing may also be performed using “alternate technology” (e.g., chromatography, mass spectrometry). Immunoassay tests typically use d-methamphetamine as the target analyte and, for federally-mandated testing, laboratories must demonstrate that ‘non-target’ analytes (e.g., d-amphetamine) with >80%-100% cross-reactivity would screen positive when tested at 125%-150% of the cutoff. There are no similar cross-reactivity requirements for the l-isomers of amphetamine and/or methamphetamine. Laboratories prefer immunoassay reagents with minimal cross-reactivity in order to avoid unnecessary confirmatory testing caused by the use of substances or medications that are not prohibited or restricted in workforce testing programs. The table below summarizes the cross-reactivity for l-methamphetamine for commonly used, FDA-listed, immunoassay systems for ‘amphetamines’: |
| | |  |
| | | | | | | As can be seen by the above table, depending upon the specific immunoassay used, the likelihood of detecting l‑methamphetamine is highly dependent not only on the metabolism, usage pattern and the specimen type, but also the testing reagent. Like most standard confirmatory assays for amphetamines, alternative initial testing technologies typically are unable to differentiate between d- and l-isomers. For example, high throughput mass spectrometry technologies (e.g., ECHO, LDTD, MALDI, Rapid Fire) are direct inlet systems and do not involve chromatographic separation while fast LC-MS/MS systems are optimized for rapid analysis and not for chromatographic separation. Consequently, if there is a question about whether d-methamphetamine was used, one cannot utilize the specificity of the initial test to help inform the decision as to whether d‑ or l-methamphetamine was used. PHARMACEUTICAL PRODUCTS There are a number of pharmaceutical preparations that are essentially prodrugs which are metabolized to methamphetamine and/or amphetamine. Of these, selegiline (Eldepryl®) is perhaps one of the most significant as it is metabolized to l-methamphetamine and, consequently, l-amphetamine. The d-isomers are not metabolites of selegiline. Other pharmaceutical products – available in the U.S. – that are metabolized to methamphetamine and/or amphetamine include: benzphetamine (Didrex®), Adderall® and Vyvanse®. For years, l-methamphetamine has been available in over-the-counter medications. The Vicks® Inhaler, and subsequent Vicks® VapoInhalerTM both contained l-methamphetamine. Despite the notable discontinuance of the Vicks® VapoInhalerTM in 2016, according to the Division of Workplace Drug Testing Programs of the U.S. Department of Health and Human Services (HHS), over-the-counter decongestant nasal inhalers containing l-methamphetamine continue to be commercially available. Current over-the-counter decongestant nasal inhalers containing l-methamphetamine contain roughly the same amount (50 mg) of l-methamphetamine as the original formulation of Vicks® Inhaler. Given the availability of over-the-counter decongestant nasal inhalers containing l-methamphetamine and prescription drugs that may be metabolized to the l-isomer, the HHS and US Department of Transportation (DOT) include discretionary ordering of d, l-isomer testing by MROs for laboratory-confirmed methamphetamine-positive test results. Federal guidance indicates that a methamphetamine concentration of more than 80% of the l-methamphetamine isomer is consistent with OTC use. Although such testing is allowed, it is not required in any federally-regulated drug testing program for methamphetamine-positive test results. However, it is generally accepted as the standard of care in federally-mandated drug testing for the MRO to order d, l-isomer testing when a donor reveals the use of an over-the-counter decongestant nasal inhaler during the verification interview. There is no mention of d, l-isomer testing under any state hair workplace drug testing statutes or requirement under other regulations. Moreover, there is no prohibition against d, l-isomer testing in any state workplace drug testing scheme. Many private-sector employers and other providers of workforce drug testing services to them consider HHS and DOT workplace drug testing provisions to represent industry standards that fill gaps in state drug testing laws applicable to private employers. It is generally accepted that d, l-isomer is also warranted for non-federal workplace drug testing where the donor claims the use of an over-the-counter decongestant nasal inhaler. In this context, employers and MROs must balance the merits of d, l-isomer testing for methamphetamine-positive laboratory test results against additional costs and increased reporting time. Unsuccessful challenges have been brought by donors challenging MRO-verified, or even laboratory-confirmed, methamphetamine-positive results reported to an employer where d, l-isomer was not performed. These legal challenges vary widely in asserted duties and facts. Some challenges have included claims that a laboratory has a duty to perform d, l-isomer testing in the absence of a test order by the designated MRO or the employer customer. These claims typically fail because a laboratory cannot be found liable for failing to provide a service for a fee that was not expressly ordered by the party responsible for paying for the service, or its designated representative. Such claims have also failed due to the position and role of a forensic drug testing laboratory, which typically has no interaction with a donor and does not receive information regarding a donor’s medical history, i.e., claimed recent use of an over-the-counter decongestant nasal inhalers. With regard to legal challenges alleging that an MRO or an employer owed a duty to a donor to order d, l-isomer testing before relying on a laboratory-confirmed methamphetamine-positive for adverse employment action, the duty analysis becomes much more problematic. The MRO is seen as the gatekeeper and safeguard for the integrity of workplace drug testing results. Therefore, where an MRO is presented with information in a verification interview for a methamphetamine-positive in a urine specimen that a donor has recently used an over-the-counter decongestant nasal inhaler, it is generally considered the standard of care to order d, l-isomer testing. Of course, this is a factually intensive determination. The donor must have actually revealed to the MRO the use of an over-the-counter decongestant nasal inhaler or some other product containing or that is metabolized to l‑methamphetamine, to justify the cost and time of additional testing of the specimen. In hair and oral fluid testing, many MROs historically may not have considered d, l-isomer testing warranted for a methamphetamine-positive result even where a donor indicates recent use of an over-the-counter decongestant nasal inhaler. This is because, as discussed above, screening assays for methamphetamine in these specimen types generally have higher specificity for methamphetamine over amphetamine and lower cross-reactivity with the l-isomers than the corresponding urine assays. With the advent of alternative initial testing technologies, the relevance and importance of d, l-isomer testing may be significantly raised. While immunoassay initial testing currently remains the standard in urine and oral fluid testing, some laboratories have begun to use alternative technology in hair testing and others may elect to adopt this technology with the advent of federally-mandated oral fluid testing. As a result of changes in technology and specimen types, MROs (or employers, although this practice itself creates legal risk for reasons outside the scope of this article) reviewing laboratory-confirmed methamphetamine-positive test results must understand the specific initial testing process and its ability to differentiate the d- and l-isomers of methamphetamine. MROs should consider ordering d, l-isomer testing when warranted by the donor’s medical history or verification interview and laboratory technology. MROs ought to ensure that, during the verification interview, the donor is questioned about recent over-the-counter drug use. MROs must also document the absence of such proffered use, to avoid claims that that d, l-isomer testing should have been ordered. | | | | | |
| | |
|
|
|---|
| |
| | | | | | | | | Michael A. Peat, Ph.D. - Forensic Toxicology Consultant ____________________________________________ |
| | | On April 27th, 2022 SAMHSA issued a notice of proposed revisions to the HHS Mandatory Guidelines for Federal Workplace Drug Testing Programs using Urine (henceforth referred to as UrMG)[1]. The SAMHSA Guidelines cover Federal employees only, however, they are normally incorporated into the DOT Drug Testing program and other mandated testing programs. These are the first proposed changes for a number of years. As is normal for proposed changes comments were invited and the closing date for these was June 6, 2022. These changes include: - Revising the definition of a substituted specimen and establishing a process to use a biomarker testing protocol.
- Revising the confirmation cut-off for morphine.
- Revising the Medical Review Officer (MRO) review process for positive codeine and morphine specimens.
- Requiring MROs to submit semi-annual reports.
I will spend more time on the first three bullets as the fourth is an administrative one. BIOMARKER PANEL The SAMHSA UrMG define a biomarker as “..an endogenous substance used to validate a biological specimen". The purpose of a biomarker test is to determine whether a submitted specimen is a human specimen. Today certified laboratories are allowed to test for biomarkers if requested by the MRO. However, if the biomarker is absent or at a concentration that is less than expected the laboratory must report the specimen as invalid. It cannot be reported as substituted. The proposed UrMG will allow these specimens to be reported as substituted, and to only allow authorized biomarker tests to be used. The UrMG will set-up an approval process for biomarker tests based on a similar process to that used to add drug and drug metabolites to the testing panel, and the biomarker panel will be approved and published by SAMHSA. This biomarker panel can then be used for testing urine specimens without an MRO request and allow specimens to be reported as substituted if the test results are abnormal. A laboratory’s proficiency in biomarker testing will be evaluated by the National Laboratory Certification Program (NCLP), as is done for other testing performed by a certified laboratory. The UrMG indicates that the current testing requirements for adulterated and substituted specimens will remain in place and the MRO role in reviewing these will also remain. CHANGES IN THE MORPHINE CONFIRMATION CUT-OFF AND THE MRO REVIEW PROCESS FOR CODEINE AND MORPHINE It might be useful at this point to remind everyone of the current steps in this process: - Specimens are screened for morphine and codeine using a cut-off of 2,000 ng/mL.
- If presumptive positives, specimens are confirmed using cut-offs of 2,000 ng/mL for each.
- If the confirmation results are below 2,000 ng/mL the laboratory will report the specimen as negative for that opiate.
- Positive specimens are reviewed by the MRO and if either morphine and/or codeine are above 15,000 ng/mL and there is no reasonable explanation the donor is reported as positive for the opiate(s) to the Designated Employer Representative (DER).
- The difficulty comes when the opiate result is between 2,000 and 15,000 ng/mL. Unless the donor has “clinical signs of opiates use” these cases are reported to the DER as negative.
This administrative cut-off of 15,000 ng/mL was included in the protocol to minimize the chances of poppy seed use causing a morphine positive between 2,000 and 15,000 ng/mL. SAMHSA is proposing to increase the confirmation cut-off for morphine to 4,000 ng/mL and to eliminate the administrative cut-off of 15,000 ng/mL. They provide documentation and peer-reviewed references (please see pages 20562 and 20563 in the UrMG[1] for the citations) to support this. Here is my summary of the information provided: - Abstention from heroin use – Studies suggest that urine concentrations of morphine are often below 15,000 ng/mL and 6-AM is absent.
- Chronic pain patients being administered heroin – patients with positive 6-AM results had morphine concentrations averaging 85,000 ng/mL with 25% at or below 10,000 ng/mL and an additional 15% falling between 10,000 and 20,000 ng/mL.
- Patients seeking in-patient addiction treatment – in 20 patients without 6-AM positive urines the morphine concentrations ranged from less than 100 to approximately 35,000 ng/mL. Only 30% of the subjects had morphine concentrations above 15,000 ng/mL. Lowering the cut-off to 4,000 ng/mL identified another 30% of the patients.
- Poppy seed food products – literature is consistent that regular ingestion of such products rarely results in urine morphine concentrations above 2,000 ng/mL. Results after reasonable consumption of poppy seed products reported morphine concentrations ranging between 160 and 3,000 ng/mL with codeine ranging between 11 and 390 ng/mL.
- Poppy seed products use that may result in concentrations above 4,000 ng/ml – SAMHSA cites a very limited number of studies where this has been reported and mentioned that the authors reported that some subjects became ill due to the large amount of poppy seeds.
- Other studies - confirmed that morphine concentrations above 4,000 ng/mL“… would be very rare, transient, and a consequence of unrealistic and extreme poppy seed exposure".
SAMHSA is confident that changing the laboratory morphine confirmation cut-off to 4,000 ng/mL and eliminating the administrative cut-off of 15,000 ng/mL will not result in an increase in morphine positives from poppy seed use. In fact, it makes the SAMHSA cut-offs for opiates identical to those used by the Department of Defense. In summary, SAMHSA presents a strong case for changing the morphine cut-off and the protocol for MRO review of positives and I would expect little comment on this from a lab perspective. However, absent any details on a biomarker testing panel it is very difficult to comment on the impact of that addition. References [1]Federal Register vol 87, no 67, April 2022 20560 – 20605 ____________________________________________ Public comments on proposed changes can be reviewed at
https://www.regulations.gov/docket/SAMHSA-2022-0002. |
|
|
|
|---|
| |
| | | | | | | | | | | | | | | Forensic drug testing programs should be justifiably concerned about the ability to accurately interpret the results of urine drug tests that are found to be either “dilute” or to have lower than average concentration. Are donors attempting to mask drug/alcohol use and/or compromise the integrity of the testing program by intentional acts of specimen dilution? Or is this dilution caused by normal physiological processes that vary from donor to donor? Let’s review what it means when a result is reported as dilute. As you remember from your MRO training courses, the concentration of urine specimens is measured using 2 values: creatinine and specific gravity. Creatinine is a protein found in all human urine caused by the normal metabolism of muscle tissue. Specific gravity is a measure of the density of the specimen as it compares to water. The average creatinine concentration nationally is 130 mg/dL (range 100 mg/dL-150 mg/dL). The lowest acceptable creatinine concentration in forensic testing is 20 mg/dL. Specific gravity is not measured in specimens until the creatinine value drops below this number, and the lowest acceptable specific gravity value is 1.0030. When both the creatinine and the specific gravity levels are below acceptable range, the specimen is labelled as ‘dilute’. These values were originally chosen by SAMHSA and have not changed. Please notice that there is a considerable range of possible concentration values that are less than average but still higher than dilute. As specimen concentration varies, so does the concentration of drug and alcohol in that specimen. The lower the concentration of the specimen, the lower the concentration of drug and alcohol that is in that specimen, and the lower the likelihood of the laboratory finding that drug or alcohol. Studies have been conducted in specimens of lower but not dilute creatinine levels where those levels were mathematically corrected to a value of 100 mg/dL. Those specimens were then sent to confirmation and tested at the higher concentration. The results were an increase in the percentage of positive results of as high as 105% for some drugs when tested at a creatinine concentration of 100 mg/dL. It is fair to say that testing of any specimen with a creatinine concentration of less than average has a lower chance of finding drug or alcohol in that specimen than if the specimen had been within average range. This is good to remember in workplace testing programs. In non workplace testing such as the testing monitoring programs conduct, strategies should be developed that take the increased likelihood of false negatives into account. These strategies might include the lowering of cutoff levels, the direct observation of specimen collection, the appropriate random mixing of alternative specimens into the testing program, and the follow-up evaluation of low creatinine and dilute specimens such as that conducted by the Nuclear Regulatory Commission (see #5 toward end of article). Forensic drug testing programs have been conducted for over 30 years and donors have become increasingly knowledgeable about the drug testing process and how to devise means to compromise that process. However some people do physiologically produce specimens of lower concentration than others do. It is not correct to assume that all low concentration specimens are the results of attempts to compromise the testing program. Dietary practices, including intake of water or other fluids as part of a healthy lifestyle can produce dilute urine specimens. It is difficult to distinguish “intentional water-loading” several hours prior to a specimen collection from a regular regime of significant fluid intake. If working with a monitoring program, one important thing to look for is any significant change in creatinine and specific gravity from one specimen to another. Ongoing regular hydration may be expected to produce ongoing regular creatinine and specific gravity values however these values do fluctuate during the day to some degree. Significant changes between specimens are not always signs of “intentional water-loading”, but they still warrant evaluation because the testing is less accurate in specimens of lower concentrations. Programs need to take that into account. Here are some general guidelines for handling low creatinine and specific gravity values: - Specimens reported as negative with creatinine 5-20 mg/mL AND specific gravity >1.0010 and <1.0030—should be considered negative dilute. If the program wants to require a re-collection of the specimen it should be done as soon as practical and with no prior notice to the participant.
- DOT specimens reported as negative with creatinine between 2 and ≤5 mg/dL AND specific gravity >1.0010 and <1.0030, should follow DOT regulations requiring an immediate observed re-collection. For non DOT specimens, these results should be reviewed and interpreted by an MRO. If the collection was not observed, an immediate re-collection under direct observation should be performed. If possible, consideration might also be given to requiring an alternative specimen collection for testing. Data shows that it is highly unlikely that dietary practices, fluid intake or physiological conditions will produce urine specimens with creatinine in the 2-5 mg/dL range. Collectors may also be interviewed to aid in determining whether this is a circumstance of an attempt to defraud or subvert the testing program.
- Specimens with creatinine <2 mg/dL AND specific gravity ≤1.0010 or ≥1.0200 are considered substituted – they are not physiologically consistent with normal human urine. The donor should be interviewed by an MRO and if no reasonable medical explanation is found these specimens should be considered a refusal to test.
- Specimens with creatinine <2 mg/dL AND specific gravity >1.0010 and <1.0200 are considered to be creatinine/specific gravity mismatches and are reported as invalid. These specimens are highly suspect and some manipulation by the participant is considered likely but is not able to be forensically proven. MRO review is recommended. If the collection was not observed, an immediate re-collection under direct observation should be performed, and/or alternative specimen testing should be considered.
- Lastly, the Nuclear Regulatory Commission (NRC) has a protocol where the laboratory reviews the immunoassay screening results to see if any data are present below cutoff. If data exist at 50% of the cutoff or higher, a separate aliquot is sent directly to confirmation for that presumptive result at the laboratory Limit of Detection (LOD).
|
| | |
| |
|
|---|
| |
| | | | | | | | | | | | | | | On April 7, 2022 the Department of Health and Human Services (HHS) published proposed changes to the Mandatory Guidelines for Federal Workplace Drug Testing Programs using Oral Fluid (OFMG) and Urine (UrMG). Comments to the changes were accepted through June 6, 2022. These Guidelines apply to 1.5 million federal employees in safety sensitive or security critical positions. The following changes are being proposed to the OFMG to catch up with current drug testing practice and technical advances: ESTABLISH A PROCESS TO PUBLISH THE HHS AUTHORIZED DRUG TESTING PANEL. For both urine and oral fluid testing, HHS is proposing that they be allowed to change the drug testing panel as necessary to keep up with current drug use trends. The time required to revise the Guidelines through the Federal review process has impeded the HHS’s ability to respond to drug use as it can take several years to do so. The HHS proposes to publish the drug testing panel in the Federal Register on at least an annual basis, including any revision to the panel without the need to undergo notice and comment. Changes to analytes and cutoffs will be based on a thorough review of relevant information, including the current state of the science, laboratory capabilities, cost associated with the change, and benefits of the change to Federal agencies. The notice would include effective dates of the drug testing panel. REVISE THE DEFINITION OF A SUBSTITUTED SPECIMEN TO INCLUDE SPECIMENS WITH A BIOMARKER CONCENTRATION INCONSISTENT WITH THAT ESTABLISHED FOR A HUMAN SPECIMEN. A biomarker is an endogenous substance used to validate a biological specimen. The purpose of a biomarker test is to determine whether a submitted specimen is a human specimen. The current OFMG (effective January 1, 2020) allow additional specimen validity testing using biomarkers upon MRO request, to provide information to assist the MRO in the verification process. The current OFMG also require HHS-certified laboratories to report a specimen as invalid when the biomarker is not present or when its concentration is not consistent with that established for human oral fluid but does not allow these specimens to be reported as substituted. The proposed Guidelines propose to revise the OFMG to define such specimens as substituted, and to allow only biomarker tests that have been authorized by SAMHSA for use in Federal agency workplace drug testing programs. ESTABLISH A PROCESS FOR HHS PUBLISHING AN AUTHORIZED BIOMARKER TESTING PANEL. To ensure that scientifically valid biomarker tests, analytes, and cutoffs are standardized for Federal workplace drug testing, HHS will institute an approval process for biomarker tests, based on review of data from the scientific and/or medical literature, before authorizing the use of the biomarker test. HHS will accept scientific information submitted for review from various sources (e.g., HHS-certified test facilities, drug testing industry stakeholders, researchers). The Department will include the authorized biomarker testing panel (i.e., a table of authorized biomarkers, with test analytes and cutoffs), in the FRN to be published each January (as described earlier in this preamble). Federal agencies may choose to test some or all of their workplace specimens for one or more authorized biomarkers. UPDATE AND CLARIFY THE ORAL FLUID COLLECTIONS PROCEDURES. Under the proposed changes, oral fluid specimen tubes would need to be sufficiently transparent to enable a visual assessment of the contents without opening the tube. This will allow collectors to identify oral fluid specimens with abnormal physical characteristics and take appropriate action (e.g., recollection). They also added a requirement for an expiration date to be included on each specimen tube. The collector will need to check the expiration date of each device prior to use and document it on the CCF. The laboratory accessioner will be required to document the expiration date on both A and B specimen tubes upon receipt. Under the proposed changes, if a specimen is collected with an expired device, laboratories are required to reject the oral fluid specimen. The revisions also include changes to the collection process to help deter donor attempts to adulterate or substitute the specimen. Collectors would need to inspect the contents of the donor’s pockets if the donor is not under direct observation throughout the entire collection. If the donor refuses, the collection continues, but the collector must keep donor under their direct observation. This is not considered a refusal to test. If the donor fails to remain at the collection site until the collection is complete, this will be reported as a refusal to test and it is the collector’s responsibility to advise the donor of this rule. To deter donor attempts to tamper with the specimen, the HHS is proposing the donor be required to wash their hands with the collector observing and to keep their hands in view and avoid touching anything after handwashing. If a donor refuses to wash their hands, it is considered a refusal to test. In addition, in an attempt to deter tampering with a specimen, the specimen collection device is to be opened by the collector in the presence of the donor. REVISE THE MEDICAL REVIEW OFFICER (MRO) VERIFICATION PROCESS FOR POSITIVE CODEINE AND MORPHINE SPECIMENS. Under current HHS OFMG, when a donor has no legitimate medical explanation for a positive codeine or morphine result equal to or greater than 150 ng/mL, the MRO reports the specimen as positive to the agency. When a donor has no legitimate medical explanation for a positive codeine or morphine result less than 150 ng/mL, the MRO must determine that there is clinical evidence of illegal opioid use (in addition to the test results) to report such specimens as positive. If the MRO finds no clinical evidence of illegal opioid use, the MRO verifies the opiate results as negative. The HHS is maintaining 150 ng/mL as the decision point but are proposing to remove the requirement for the MRO to report specimens with morphine and/or codeine between the cutoff and 150 ng/mL as positive based on clinical evidence of illicit drug use. Because MROs generally are not conducting donor interviews in-person, there are concerns over the feasibility of the current requirement to make a clinical assessment (i.e., physical examination) of the donor. In consideration of this, the HHS determined that the additional requirement for clinical evidence of illegal opioid use is no longer practical or effective. Under the proposed changes, the MRO will verify such specimens as negative unless the donor admits to illegal opioid use that could have caused the positive result. The revised procedures is based on current scientific information and industry practice and should provide a reliable and objective basis for identifying illicit drug use. REQUIRE MROS TO SUBMIT SEMIANNUAL REPORTS TO THE HHS SECRETARY ON FEDERAL AGENCY SPECIMENS THAT WERE REPORTED AS POSITIVE FOR A DRUG OR DRUG METABOLITE BY A LABORATORY AND VERIFIED AS NEGATIVE BY THE MRO. HHS is proposing to require each MRO performing medical review services for Federal agencies to submit semiannual reports in January and July of each year that would include Federal agency specimens that were reported as positive for a drug or drug metabolite by the laboratory, and verified as negative by the MRO, along with the reason for the negative verification (e.g., a valid prescription). The reports will not contain any personally identifiable information of the donors. This revision will enable the HHS oversight of MRO reporting practices and enhance the HHS’s ability to verify the accuracy of MRO reports and address areas of confusion about the Mandatory Guidelines requirements. To facilitate report preparation and review, HHS will include a template for these MRO reports in the MRO Guidance Manual and will arrange a secure method for MROs to submit reports electronically. ADDITIONAL CHANGES: Some wording changes have been made for clarity and for consistency between the UrMG and OFMG. ____________________________________________ Public comments on proposed changes can be reviewed at
https://www.regulations.gov/docket/SAMHSA-2022-0001 |
| | | | |
| |
|
|---|
| |
| | | | | | | | | ODAPC - DOT SAMHSA - HHS NRC CUSTODY AND CONTROL FORMS (CCFs) | | |
| | | | |
| |
|
|---|
|
| | | | | | | |
 | | | | |
| | | |
 | | | | |
| | | |
 | | | | |
|
|---|
| |
|
|
|
|
|
|---|
| | |
| | | | | | | Medical Review Officer Certification Council (MROCC) 3231 S Halsted St, Ste Front #167
Chicago, IL 60608
Tel: 847.631.0599
Email: mrocc@mrocc.org |
|
|
| Editor:James Ferguson, DO Managing Editor: Kristine Pasciak Copyright 2022 Medical Review Officer Certification Council ISSN: 2833-0870 |
|
|
|
|---|
| |
| | | | | | | MRO Quarterly is an educational publication intended to provide information and opinion to health professionals. The statements and opinions contained in this document are solely those of the individual authors/contributors and not MROCC. MROCC and its editorial staff disclaim responsibility for any injury to persons or property resulting from any ideas or products referred to in this newsletter. To unsubscribe from MROCC emails, please send an email |
|
|
|
|---|
| | | | | |
|
|